Policy Brief:
A Disability-Inclusive
Response to COVID-19
M AY 2 0 2 0
1. Executive Summary
The global crisis of COVID-19 is deepening
pre-existing inequalities, exposing the
extent of exclusion and highlighting that
work on disability inclusion is imperative.
People with disabilities—one billion people—
are one of the most excluded groups
in our society and are among the hardest
hit in this crisis in terms of fatalities.
Even under normal circumstances, persons
with disabilities are less likely to access health
care, education, employment and to participate
in the community. They are more likely to live
in poverty, experience higher rates of violence,
neglect and abuse, and are among the most
marginalized in any crisis-affected community.
COVID-19 has further compounded this
situation, disproportionately impacting persons
with disabilities both directly and indirectly.
An integrated approach is required to ensure
that persons with disabilities are not left
behind in COVID-19 response and recovery.
It calls for placing them at the centre of the
response, participating as agents of planning
and implementation. All COVID-19 related
action must prohibit any form of discrimination
based on disability and take into consideration
the intersections of gender and age, among
other factors. This is necessary effectively
and eciently to address and prevent barriers
that may arise during response and recovery.
Disability inclusion will result in a COVID-
19 response and recovery that better
serves everyone, more fully suppressing
the virus, as well as building back better. It
will provide for more agile systems capable
of responding to complex situations,
reaching the furthest behind rst.
This Policy Brief highlights the impact of COVID-
19 on persons with disabilities and in doing so,
outlines key actions and recommendations
to make the response and recovery inclusive
of persons with disabilities. While the brief
contains specic recommendations focusing
on key sectors, it identies four overarching
areas of action that are applicable for all.
1. Ensure mainstreaming of disability in all
COVID-19 response and recovery together
with targeted actions. A combination of
mainstream and disability-specic meas-
ures are necessary to ensure systematic
inclusion of persons with disabilities.
2. Ensure accessibility of information,
facilities, services and programmes in
the COVID-19 response and recovery.
Accessibility is fundamental to the inclusion
of persons with disabilities in the immediate
health and socio-economic response to
COVID-19. If public health information, the
built environment, communications and
2 POLICY BRIEF: A DISABILITY-INCLUSIVE RESPONSE TO COVID-19

technologies, and goods and services are
not accessible, people with disabilities
cannot take necessary decisions, live
independently and isolate or quarantine
safely, or access health and public
services on an equal basis with others.
3. Ensure meaningful consultation with
and active participation of persons with
disabilities and their representative
organizations in all stages of the
COVID-19 response and recovery.
Persons with disabilities have important
contributions to make in tackling the
crisis and building the future. Many
persons with disabilities have experience
of thriving in situations of isolation and
alternate working arrangements that
can offer models for navigating the
current situation. Perspectives and lived
experiences of disability contribute
to creativity, new approaches and
innovative solutions to challenges.
4. Establish accountability mechanisms
to ensure disability inclusion in the
COVID-19 response. Ensure inclusive
investments to support disability-inclusive
outcomes. Governments, donors, UN
agencies and other actors need to establish
mechanisms to monitor investments
to ensure it is reaching persons with
disabilities. Disaggregating data by
disability is key to ensure accountability.
Inclusion of persons with disabilities in the
COVID-19 response and recovery is a vital part
of achieving the pledge to leave no one behind,
and a critical test of the global commitments
of the Convention of the Rights of Persons
with Disabilities (CRPD), the 2030 Agenda
for Sustainable Development, the Agenda for
Humanity and the United Nations Disability
Inclusion Strategy. It is also central to the
UN’s commitment to achieve transformative
and lasting change on disability inclusion.
POLICY BRIEF: A DISABILITY-INCLUSIVE RESPONSE TO COVID-19 3
2. How COVID-19
impacts persons
with disabilities
Persons with disabilities are
disproportionately impacted by the COVID-
19 outbreak. An estimated 46% of older
people aged 60 years and over are people
with disabilities.
1
One in every ve women
is likely to experience disability in her
life, while one in every ten children is a
child with a disability.
2
Of the one billion
population of persons with disabilities,
80% live in developing countries.
3
They represent a diverse population of people
with different impairments and support
requirements, who face signicant barriers
in exercising their rights throughout the
lifecycle. Some groups face even greater
marginalization—for example persons with
intellectual and psychosocial disabilities,
persons who are deafblind—who are more
likely to be excluded from services, live or
be detained in institutions, and experience
higher rates of violence, neglect and abuse.
As the report ‘Shared Responsibility, Global
Solidarity’ on the socio-economic impact
of the pandemic reects, COVID-19 is
not simply a health crisis—it is attacking
societies at their core.
4
The response is
feeding on pre-existing social and economic
inequalities associated with disability and
threatens to exacerbate them further.
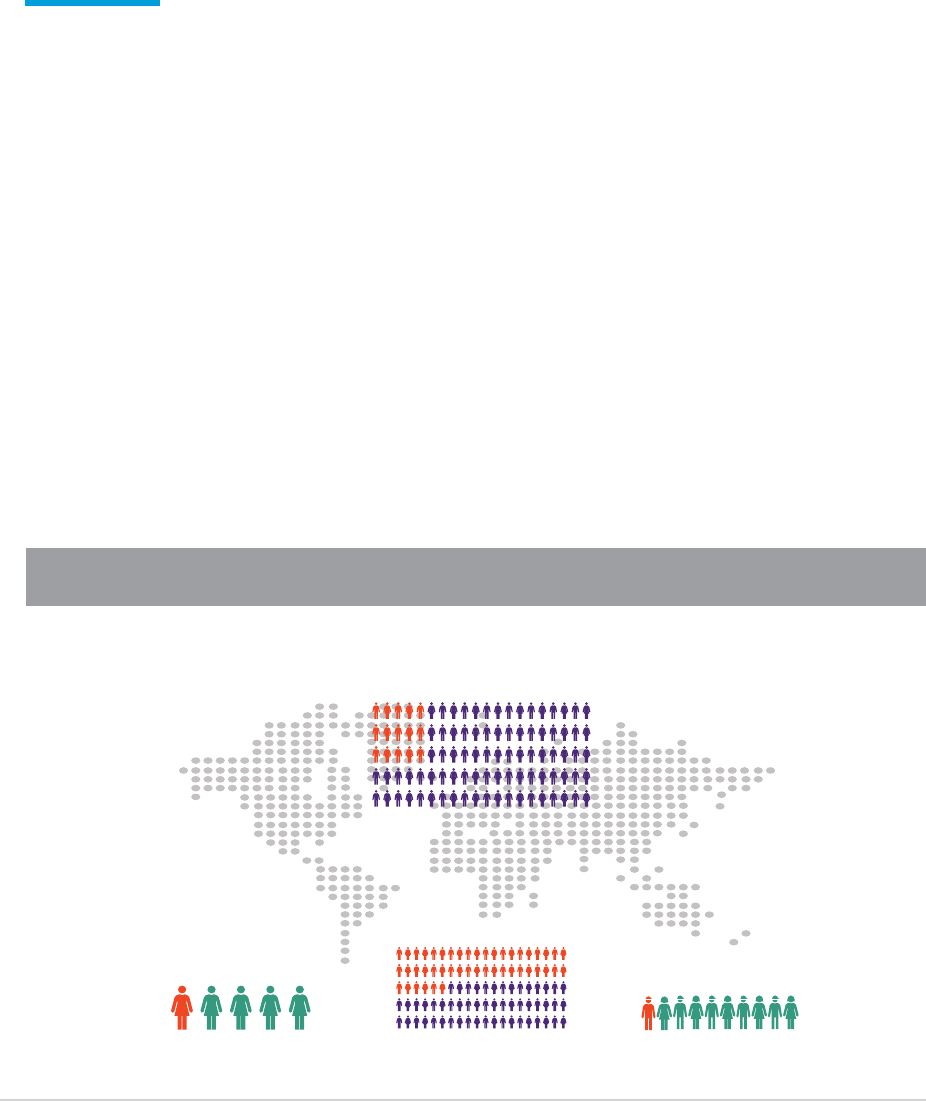
GLOBAL POPULATION OF PERSONS WITH DISABILITIES
Figure 1 Global population of persons with disabilities (IASC Guidelines, 2019, Inclusion of Persons with Disabilities in Humanitarian Action)
4 POLICY BRIEF: A DISABILITY-INCLUSIVE RESPONSE TO COVID-19
2
1. Introduction
Why are the guidelines important?
1
W HO and World Bank,
World Report on Disability
(2011).
2
R eport of the United Nations Secretary-General for the World Humanitarian Summit,
One Humanity, Shared Responsibility
.
3
K atsunori Fujii, ‘
The Great East Japan Earthquake and Disabled Persons
’, in
Disability Information Resources
, Japan.
4
U NICEF,
Including children with disabilities in humanitarian action – General Guidance
(2017).
5
Sources: WHO and World Bank,
World Report on Disability
(2011); UN DESA,
Ageing and Disability
; UNICEF,
Children and Young People
with Disabilities
(2013).
Persons with disabilities are estimated to represent
15 per cent of the world’s population.
1
In humanitarian
contexts, they may form amuch higher percentage.
They are among the most marginalized people in
crisis-affected communities
2
and are disproportion-
ately affected by confl ict and emergency situations.
In disasters, their mortality rate is two to four times
higher than that of persons without disabilities.
3
Persons with disabilities are not ahomogeneous
group. They are diverse in their experience, in the
ways that attitudinal, physical and communication
barriers impede their participation and inclusion in
humanitarian action, and in their identity, including
their age, gender, ethnicity, location and race. Due to
the intersectionality of these factors, persons with
disabilities face greater marginalization and discrim-
ination. During humanitarian crises, for example, chil-
dren with disabilities are at higher risk of abuse and
neglect, and women with disabilities are at higher
risk of sexual violence.
4
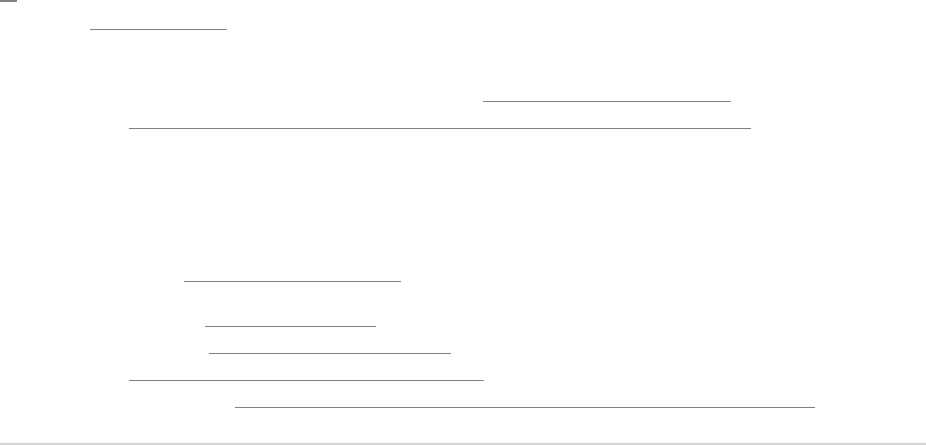
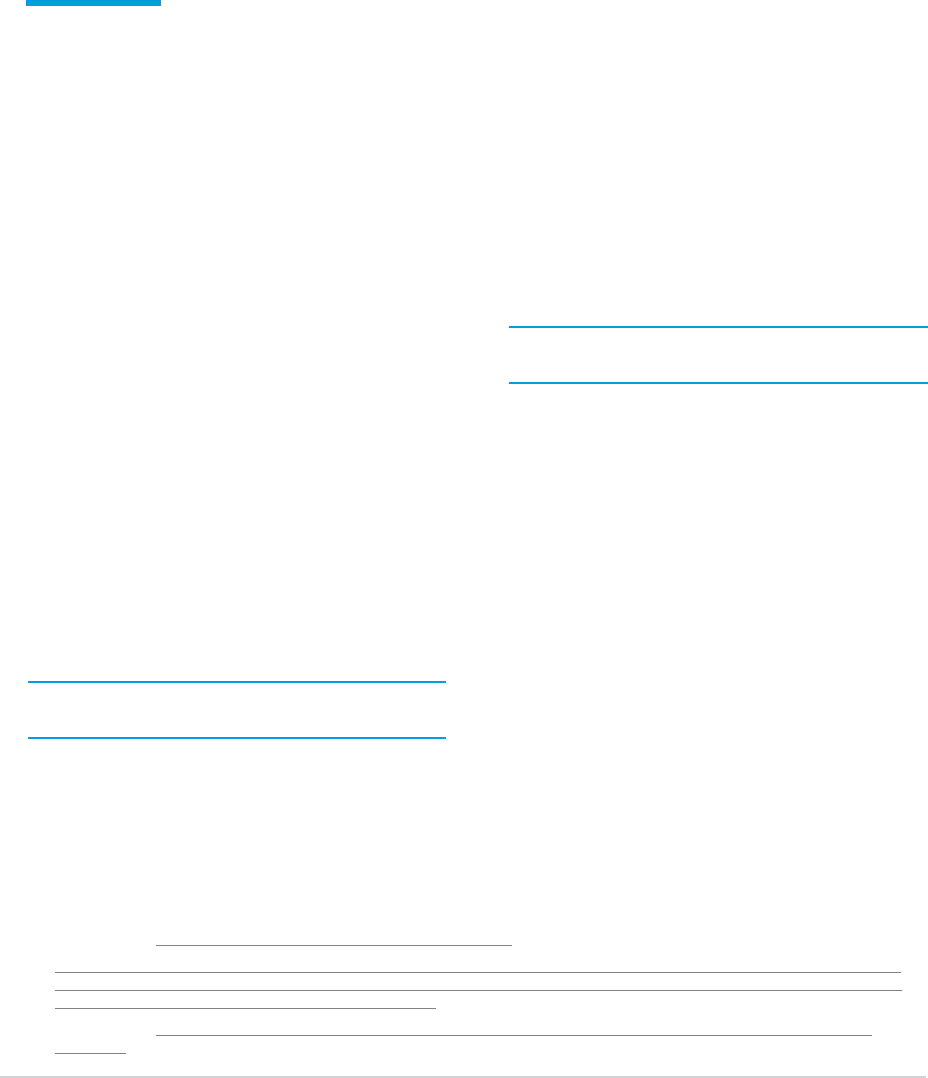
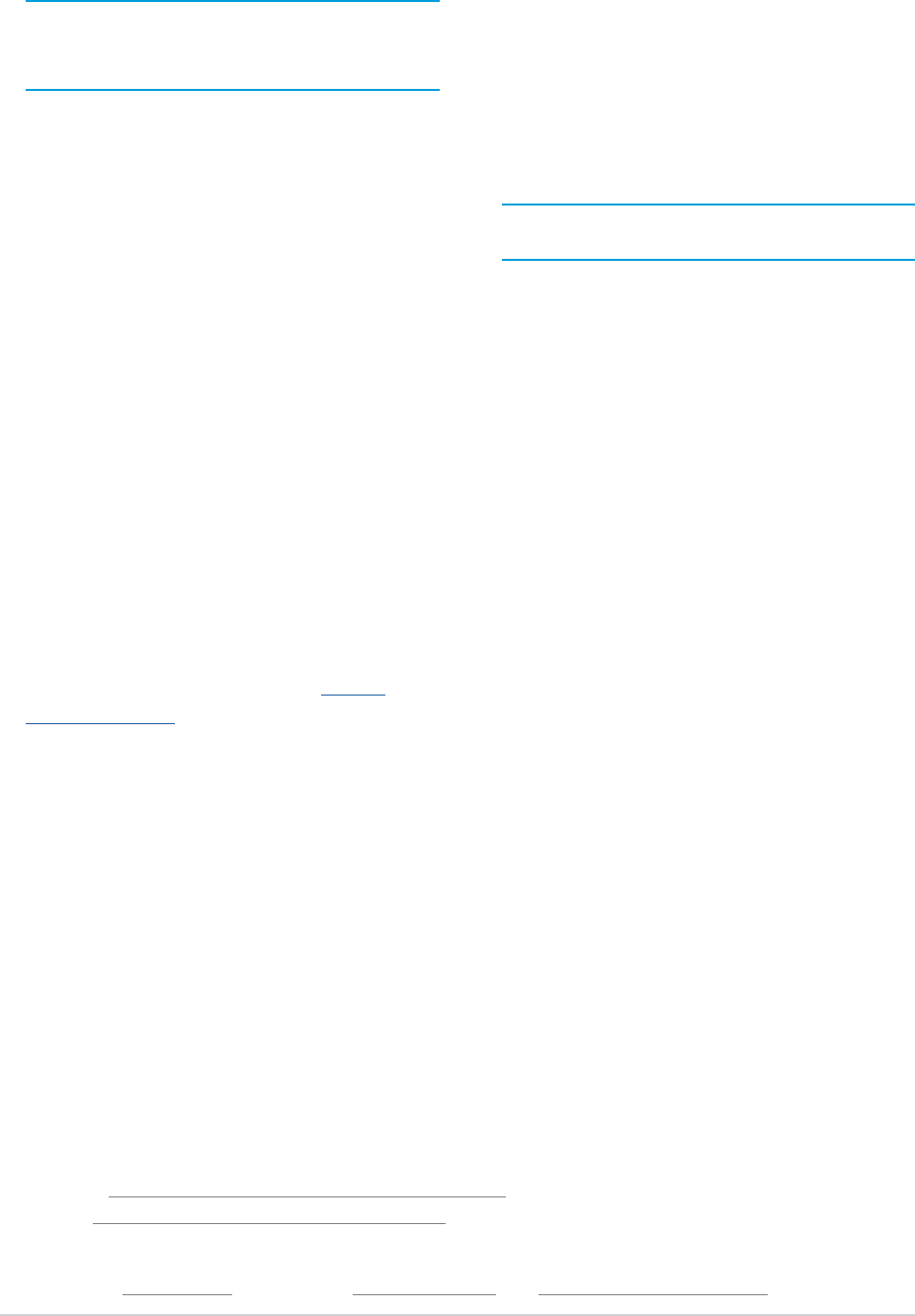
Diagram 2 | Global population of persons with disabilities
5
15%
An estimated 15% of the world’s population have adisability.
1 in 5
One in fi ve women is
likely to experience
disability during her life.
46%
46% of persons aged 60 years
and over have adisability.
1 in 10
One in ten children is
achild with adisability.
Persons with disabilities are at greater risk of
contracting COVID-19. They may experience
barriers to implement basic protection measures
such as hand-washing and maintaining
physical distancing for several reasons: lack of
accessibility of water, sanitation and hygiene
(WASH) facilities; a reliance on physical contact
to get support; inaccessibility of public health
information; or being placed in institutional
settings which are often overcrowded and
unsanitary.
5
These barriers are exacerbated
for those living in informal settlements and/
or affected by humanitarian emergencies.
Persons with disabilities are at greater risk of
developing more severe health conditions and
dying from COVID-19. They have greater health
requirements and poorer health outcomes.
For example, they are more susceptible to
secondary conditions and co-morbidities, such
as lung problems, diabetes and heart disease,
and obesity, which can worsen the outcome of
COVID-19 infections.
6
The barriers to accessing
healthcare are further exacerbated during the
COVID-19 crisis, making timely and appropriate
care dicult for persons with disabilities.
Persons with disabilities living in institutions
are more likely to contract the virus and
have higher rates of mortality. Persons
with disabilities, including older people
with disabilities, represent the majority of
institutionalized people globally.
7
People with
disabilities are also overrepresented in the prison
population, particularly persons with intellectual
and psychosocial disabilities.
8
People in
institutional settings, such as nursing homes
9
,
social care homes and psychiatric facilities, as
well as detention facilities and penitentiaries
10
,
experience signicant barriers to implement
basic hygiene measures and physical distance,
and have limited access to COVID-19-related
information, testing and healthcare. Emerging
evidence indicates that people in institutional
settings are experiencing the highest rates of
infection and mortality from COVID-19.
11
The
percentage of COVID-19 related deaths in care
homes—where older persons with disabilities
are overrepresented—ranges from 19% to 72%
in countries in which ocial data is available.
12
Persons with disabilities are at greater risk
of discrimination in accessing healthcare
and life-saving procedures during the COVID-
19 outbreak. In some countries, health care
rationing decisions, including triage protocols
POLICY BRIEF: A DISABILITY-INCLUSIVE RESPONSE TO COVID-19 5
1 UN DESA Disability and Ageing
2 WHO and World Bank, World Report on Disability (2011); UN DESA, Ageing and Disability; UNICEF, Children and Young People with
Disabilities (2013).
3 United Nations Department of Economic and Social Affairs (UN DESA), Factsheet on Persons with Disabilities
4 United Nations, Shared Responsibility, Global Solidarity: Responding to the Socio-Economic Impacts of Covid-19, March 2020
5 WHO, Disability considerations during the COVID-19 outbreak, 2020; H. Kuper & P. Heydt, The Missing Billion, access to health services
for 1 billion people with disabilities, LSHTM, 2019; I. Mactaggart et al. (2018), Access to water and sanitation among people with
disabilities, BMJ open vol. 8(6), e020077.
6 WHO, World Report on Disability, 2011; A. K. Singh et al. (2020), “Comorbidities in COVID-19: Outcomes in hypertensive cohort and
controversies with renin angiotensin system blockers”, Diabetes & metabolic syndrome 14(4).
7 OECD Health Statistics 2019, Beds in residential long-term care facilities, Long-term care beds in hospitals and Psychiatric care beds
in hospitals, available at https://oe.cd/ds/health-statistics; M. Luppa et al (2010), “Prediction of institutionalization in the elderly. A
systematic review”, Age Ageing 39(1).
8 Penal Reform International, Global Prison Trends 2020
9 United Nations, Policy Brief: Impact of COVID-19 on Older Persons, May 2020
10 United Nations, COVID-19 and Human Rights: We are all in this together, April 2020
11 A. Comas-Herrera et al. (2020), “Mortality associated with COVID-19 outbreaks in care homes: early international evidence”
6 POLICY BRIEF: A DISABILITY-INCLUSIVE RESPONSE TO COVID-19
(e.g. intensive care beds, ventilators), are
not being based on an individual prognosis,
but rather on discriminatory criteria, such as
age or assumptions about quality or value of
life based on disability.
13
Moreover, access
to healthcare, rehabilitation and assistive
technologies for persons with disabilities,
including with respect to accessibility and
affordability,
14
can also be curtailed due to the
increased pressure on healthcare systems.
Persons with disabilities are particularly
disadvantaged by the socio-economic
consequences of COVID-19 and measures to
control the pandemic. COVID-19 has both short-
term and far-reaching implications for people
with disabilities in many areas of life, which
may be further exacerbated in humanitarian
and disaster contexts and fragile settings:
•
Impact on employment and social protec-
tion. Already facing exclusion in employ-
ment
15
, persons with disabilities are more
likely to lose their job and experience greater
diculties returning to work during recov-
ery.
16
In most countries social protection
systems offer little support to persons with
disabilities and their families with much
less access to social insurance. Only 28%
of persons with signicant disabilities have
access to disability benets globally, and only
1% in low-income countries.
17
The increased
demand for unpaid care and domestic work
in the context of the pandemic is deepening
already existing inequalities
18
which may be
exacerbated for women with disabilities.
19
•
Impact on education. While reliable gures
on students with disabilities are not yet
available, it is likely that the current crisis
has exacerbated their exclusion from educa-
tion.
20
As detailed in the policy brief on the
impact of COVID-19 on children, students
with disabilities are least likely to benet
from distance learning solutions.
21
Lack of
support, access to the internet, accessible
software and learning materials is likely to
deepen the gap for students with disabilities.
Disruption to skills and training programmes
are likely to have far-reaching effects on
youth with disabilities who face a multitude
of barriers to entering the workforce.
•
Impact on support services. For many
people with disabilities, access to support
services is essential to lead safe, healthy
and independent lives. Measures to contain
the spread of COVID-19 have resulted in
12 A. Comas-Herrera et al. (2020), “Mortality associated with COVID-19 outbreaks in care homes: early international evidence”
13 S. Bagenstos (2020), “May Hospitals Withhold Ventilators from COVID-19 Patients with Pre-Existing Disabilities? Notes on the Law and
Ethics of Disability-Based Medical Rationing”, 130 Yale Law Journal Forum (Forthcoming)
14 Baart & F. Taaka (2017), “Barriers to Healthcare Services for People with Disabilities in Developing Countries: A Literature Review”,
Disability, CBR & Inclusive Development, 28(4).
15 United Nations, Disability and Development Report, Realizing the Sustainable Development Goals by, for and with persons with
disabilities, 2018
16 Mitra, S. and Kruse, D., 2016. Are workers with disabilities more likely to be displaced?. The International Journal of Human Resource
Management, 27(14), pp.1550-1579.
17 ILO 2017 World report on social protection Universal social protection to achieve the Sustainable Development Goals; page 66-73,
ILO 2019. Measuring nancing gaps in social protection for achieving SDG target 1.3 global estimates and strategies for developing
countries UN DESA, 2017, Promoting social inclusion through social protection, Report on the World Social Situation S. Kidd et al.,
Leaving No-one Behind: Building Inclusive Social Protection Systems for Persons with Disabilities, Development Pathways, 2019.
18 United Nations, Policy Brief: The Impact of COVID-19 on Women, April 2020
19 United Nations, Disability and Development Report, Realizing the Sustainable Development Goals by, for and with persons with
disabilities, 2018
20 United Nations, Disability and Development Report, Realizing the Sustainable Development Goals by, for and with persons with
disabilities, 2018
21 United Nations, Policy Brief: The Impact of COVID-19 on Children, April 2020

22 United Nations, Policy Brief: The Impact of COVID-19 on Women, April 2020
23 UN Women, COVID-19 and ending violence against women and girls, 2020
24 L. Jones et al. (2012), “Prevalence and risk of violence against children with disabilities: a systematic review and meta-analysis of
observational studies”, The Lancet 380(9845); K. Hughes et al. (2012), “Prevalence and risk of violence against adults with disabilities:
a systematic review and meta-analysis of observational studies”, The Lancet 379(9826).
25 J. Meaney-Davis et al., The impacts of COVID-19 on people with disabilities: a rapid review, Inclusive Features, Disability Inclusion
Helpdesk Query No: 35, 2020
POLICY BRIEF: A DISABILITY-INCLUSIVE RESPONSE TO COVID-19 7
signicant disruptions to services, support
systems and informal networks, such as per-
sonal assistance, sign language and tactile
interpretation, and psychosocial support.
The economic impact of COVID-19 may
also lead to even greater cuts within exist-
ing services in the post-pandemic period.
•
Impact of violence on persons with
disabilities. The policy brief on the impact of
COVID-19 on women documents early reports
which indicate a substantial increase of
domestic violence in the midst of lockdown
measures,
22
which has a particular impact
on women and girls with disabilities.
23
Given
that both children and adults with disabilities
are at much higher risk of violence than their
peers without disabilities,
24
it can be assumed
that they are disproportionately impacted.
Increased stigma and discrimination
against persons with disabilities within
communities has also been reported.
25
8 POLICY BRIEF: A DISABILITY-INCLUSIVE RESPONSE TO COVID-19
A human rights-based approach to
disability is required to ensure persons
with disabilities are not left behind.
26
Both the CRPD and the 2030 Agenda call
for placing persons with disabilities at
the centre of all our efforts, as agents
of planning and implementation.
A combination of mainstreaming and targeted
measures is necessary in all interventions.
Persons with disabilities share the same primary
needs as everyone else: health protection
and treatment, basic services, shelter and
income. The best way to address their inclusion
is through mainstreaming disability in all
plans and efforts. Targeted measures need
to complement disability mainstreaming by
addressing specic requirements that cannot
be met by making general responses inclusive.
NON-DISCRIMINATION
Non-discrimination is a core human rights
principle. COVID-19 response and recovery
must prohibit discrimination on the basis of
disability, as well as any criteria which could
have a disproportionate impact on persons with
disabilities. It is necessary to recognise and take
measures against disadvantage experienced
by persons with disabilities by taking
proactive steps, including through reasonable
accommodation, to ensure they equally benet
from COVID-19 response measures.
27
INTERSECTIONALITY
Persons with disabilities experiencing
intersectional and multiple discrimination as
a result of their gender identity, age, ethnicity,
race, sexual orientation, origin, location and
legal status, among other factors, will carry
a heavier burden of the immediate and long-
term economic and social consequences
of the pandemic.
28
COVID-19 response
and recovery needs to reect and respond
to the multiple and intersecting forms
of discrimination faced by persons with
disabilities to ensure that the most marginalised
groups among them are not left behind.
3. Foundations for a
disability-inclusive COVID-19
response and recovery
26 United Nations, COVID-19 and Human Rights: We are all in this together, April 2020
27 Reasonable Accommodation means “Necessary and appropriate modication and adjustments not imposing a disproportionate or
undue burden, where needed in a particular case, to ensure to persons with disabilities the enjoyment or exercise on an equal basis
with others of all human rights and fundamental freedoms” (CRPD Article 2)
28 United Nations, Disability and Development Report, Realizing the Sustainable Development Goals by, for and with persons with
disabilities, 2018
POLICY BRIEF: A DISABILITY-INCLUSIVE RESPONSE TO COVID-19 9
ACCESSIBILITY
Ensuring accessibility of facilities, services
and information is fundamental to a disability
inclusive COVID-19 response and recovery. If
public health information, buildings, transport,
communications, technologies, goods and
services are not accessible, persons with
disabilities cannot take necessary decisions, live
independently and isolate or quarantine safely,
or access health and public services on an equal
basis with others. Such measures do not need to
add greatly to overall cost especially if the needs
of the maximum number of users are considered
in the initial design.
29
Research shows that if they
are considered from the design stage, ensuring
accessibility can cost as little as 1% more.
30
PARTICIPATION
Persons with disabilities have the right to
participate fully and effectively in decisions
that affect their lives.
31
They are a diverse,
non-homogenous population who possess
unique knowledge and lived experience
of disability that others do not.
Close consultation and active involvement of
people with disabilities and their representative
organizations at all stages–from planning and
design to implementation and monitoring—
is key to ensuring inclusive response.
Partnerships and collaboration will improve
effectiveness and accountability, assist in
directly achieving inclusion and ensuring
that all action related to COVID-19 benets
persons with disabilities, and contributes to
longer-term development and recovery.
ACCOUNTABILITY
Accountability is essential for ensuring that the
COVID-19 response and recovery is inclusive
and respectful of the rights of persons with
disabilities. Governments, UN entities and other
actors are accountable to affected populations,
including persons with disabilities, and
mechanisms need to be established to engage
with communities to inform programming
and adjust it according to feedback.
DATA DISAGGREGATION
To understand the different ways in which people
with disabilities experience the impact of COVID-
19, and to monitor their inclusion in all phases
of the response and recovery, ensuring the
collection and availability of disaggregated data
by disability is essential. To that end, data should
be collected using internationally recognized
methods, such as the Washington Group tools.
32
More in-depth qualitative data can be collected
through needs assessments and surveys,
such as the WHO Model Disability Survey.
For planning purposes, where primary data
collection is not undertaken or secondary data
sources on disability is not available, the World
Bank/WHO 15 per cent estimate of persons with
disabilities in the population may be used.
33
29 Universal design means the design of products, environments, programmes and services to be usable by all people, to the greatest
extent possible, without the need for adaptation or specialized design (CRPD Article 2).
30 E. Steinfeld, Education for all: the cost of accessibility, World Bank Education Notes, 2005.
31 CRPD, Article 4.3.
32 Washington Group (WG) on Disability Statistics, Questions sets,
33 WHO and World Bank, World Report on Disability (2011).
10 POLICY BRIEF: A DISABILITY-INCLUSIVE RESPONSE TO COVID-19
The following section outlines key actions
to protect persons with disabilities from
contracting COVID-19 and the impact
of lockdowns, physical distancing and
isolation measures, and to achieve a
disability-inclusive response and recovery.
HEALTH
People with disabilities are more susceptible
to contracting COVID-19, and barriers to
accessing health services, including testing,
are exacerbated during the crisis. Lockdowns
can lead to restricted access to essential
goods and medicines, as well as limit access
to supports. The disruption of wider health
services puts persons with disabilities at a
disadvantage as they may require more frequent
access due to underlying health conditions.
34
Ensure accessible public health information.
An appropriate response requires measures
to ensure that information is accessible, up to
date, and keeps pace with the rapidly changing
knowledge evidenced during the pandemic.
35
For example, Inclusion Europe has produced
information and links on COVID-19 in Easy-to-
Read format in multiple languages. Through the
joint UN Partnership on the Rights of Persons
with Disabilities (UN PRPD) programme
36
in Nepal, information on COVID-19 included
accessibility features, including sign language.
Implement protective measures against
COVID-19. Access to appropriate WASH
facilities that make frequent hand-washing
possible is essential, as is the targeted provision
of protective measures for those providing
support to persons with disabilities either at
home or in institutions. The distribution of
personal protective equipment to persons
with disabilities needs to be tailored to their
impairment. For example, given that masks
make it impossible to read lips or see facial
expressions, deaf and hard of hearing persons
will benet better from face shields.
Ensure accessibility to services. Measures
need to be put in place to facilitate the
timely access to health services for persons
with disabilities, such as transportation to
healthcare facilities, access to sign language
34 WHO and World Bank, World Report on Disability (2011).
35 United Nations, Shared Responsibility, Global Solidarity: Responding to the Socio-Economic Impacts of Covid-19, March 2020
36 UN Partnership on the Rights of Persons with Disabilities (UNPRPD) supports joint programmes by UN agencies together with
governments and organizations of persons with disabilities at country level to advance CRPD implementation. In Nepal, the UNPRPD
project is jointly implemented by UNDP, UNFPA, WHO and UN Women and partners.
4. Sectoral actions and
recommendations for a
disability-inclusive COVID-19
response and recovery
POLICY BRIEF: A DISABILITY-INCLUSIVE RESPONSE TO COVID-19 11
interpretation in hospitals, as well as the
procurement of goods, medicines and services.
Essential health services, including sexual and
reproductive health, must be accessible—for
example, ensuring telehealth programmes are
accessible for persons with disabilities who
require different modes of communication.
By way of example, the United Arab Emirates
has launched a national programme to test
persons with disabilities in their homes,
and as of mid-April, had conducted 650,000
COVID-19 tests of persons with disabilities.
Ensure non-discrimination in the allocation
of scarce medical resources. It is important
to mitigate the risk of discriminatory
decisions in resource allocation that put
people with disabilities at a high level of
disadvantage
37
by applying ethical principles
that prioritize treatment for persons in
situations of particular vulnerability.
38
Make mental health interventions inclusive of
persons with disabilities. Anxiety, lockdowns,
isolation, and information consumption, loss
of livelihoods and support systems due to
the pandemic impact on mental health of all
people, including persons with disabilities. As
documented in the policy brief on the impact of
COVID-19 on older persons, physical distancing
measures that restrict visitors and group
activities in institutions can also negatively
affect physical, as well as mental health and
well-being.
39
Mental health and psychosocial
support needs to be accessible and not
discriminate against persons with disabilities.
37 R. D. Truog et al. (2020), “The Toughest Triage — Allocating Ventilators in a Pandemic”, The New England Journal of Medicine,
DOI: 10.1056/NEJMp2005689.
38 WHO, Guidance for Managing Ethical Issues in Infectious Disease Outbreaks, 2016.
39 United Nations, Policy Brief: Impact of COVID-19 on Older Persons, May 2020
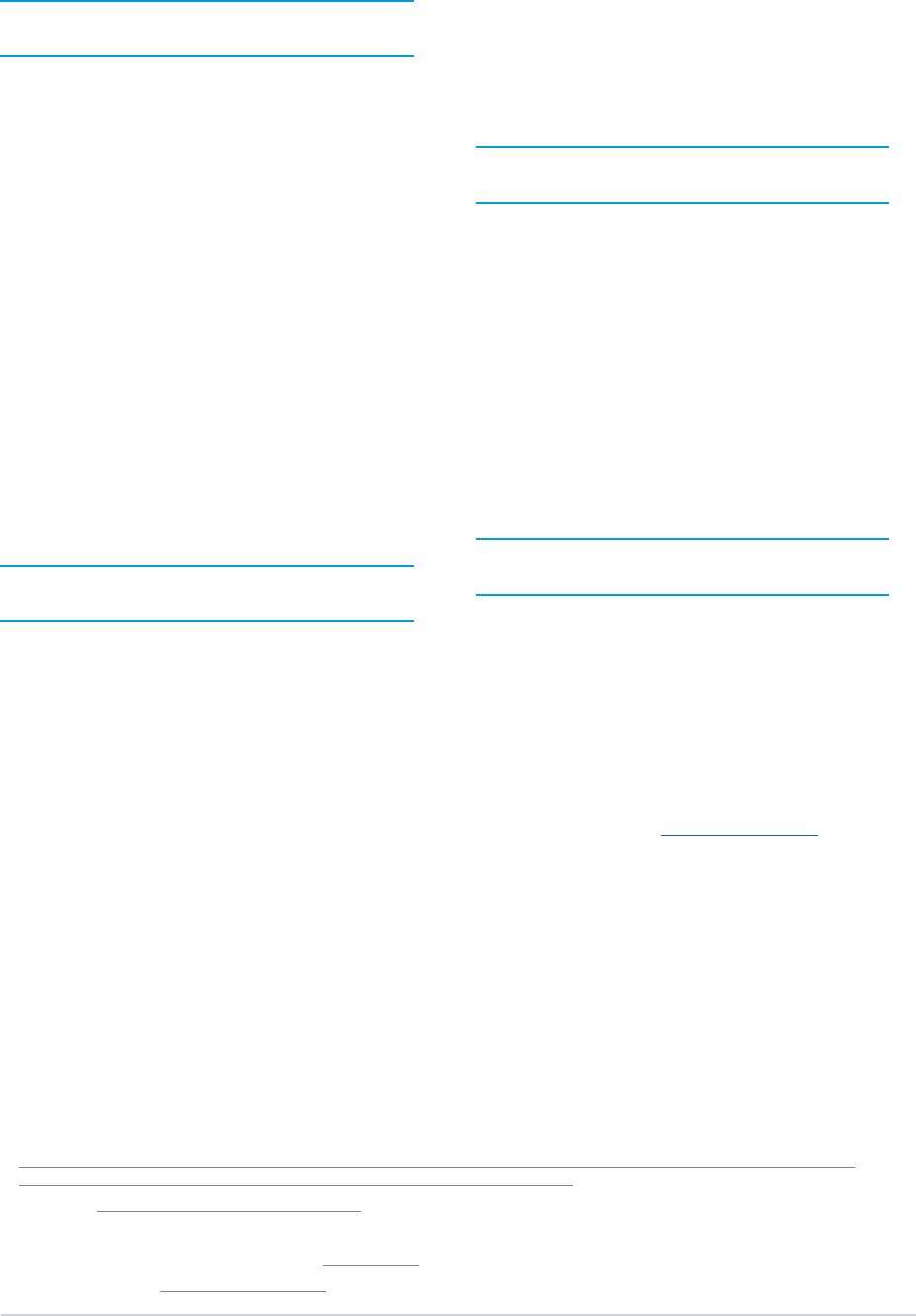
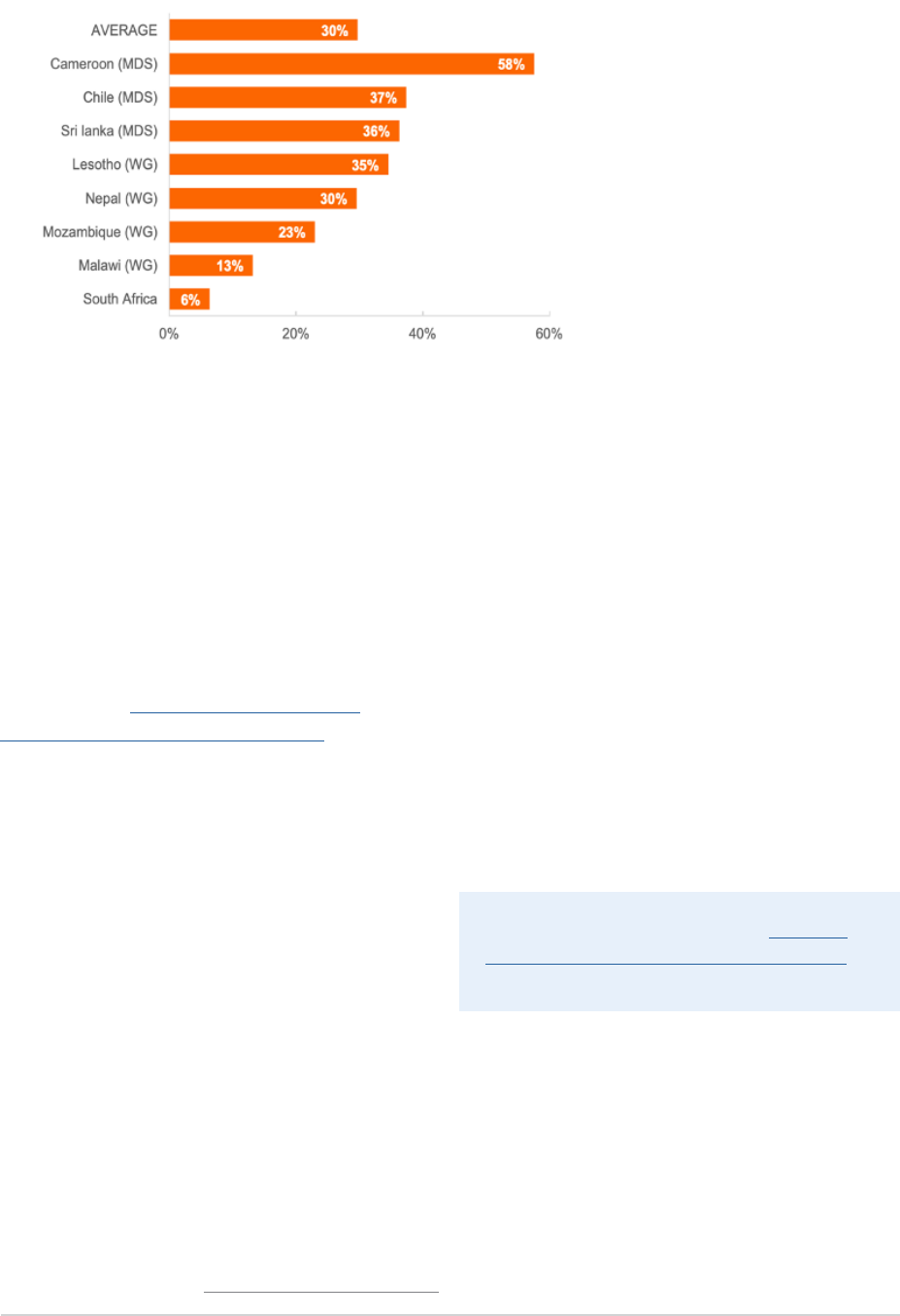
Figure 2 Percentage of persons with disabilities who report that health-care facilities are hindering or not accessible (United Nations,
Disability and Development Report, 2018)
WHO has produced guidelines on Disability
considerations during the COVID-19 outbreak.
12 POLICY BRIEF: A DISABILITY-INCLUSIVE RESPONSE TO COVID-19
PROTECTING PEOPLE IN
INSTITUTIONAL SETTINGS
Institutional settings have become COVID-19
hotspots, highlighting systemic challenges
in these settings. People with disabilities in
institutional settings face heightened risk of
contracting and dying from COVID-19. Their
situation is compounded by greater risks, such
as abuse, restraint, isolation and violence.
Prepare institutions to prevent and respond to
potential infections. This includes prioritising
testing and preventive measures within
institutions to reduce infection risks, addressing
overcrowding, isolation and physical distancing
measures among residents, modifying visiting
hours, ensuring use of protective equipment is
mandatory, and improving hygiene conditions.
It is important to guarantee that those who
contract the virus receive adequate treatment
and health care and, when needed, are
transferred to hospitals and/or emergency
care units. In Canada, for example, priority
testing guidelines have been issued with
specic measures for institutional settings.
Reduce the number of people within
institutions. It is important to take immediate
action to discharge and release persons
with disabilities from institutions, whenever
possible. Deinstitutionalization strategies
need to be accelerated and reinforced with
clear timelines and concrete benchmarks.
Reduce the number of persons with
disabilities in prisons. Whenever possible, it
will be important to explore early release and
probation or shorten or commute sentences.
Other possible measures would include
reducing the use of pre-trial detention, and
promptly ensuring support in the community
through family and/or informal networks.
40
In a number of countries around the world
prisoners with disabilities have been released.
SUPPORT SERVICES
Many persons with disabilities rely on
support services for daily living and to
participate in their communities. These
include personal assistance, sign language
and tactile interpretation, in-home services
and peer support, amongst others.
Ensure the continuity of support services.
It is important to develop and implement service
continuity plans, particularly for people with
disabilities with high support needs, as well
as measures to reduce potential exposure to
COVID-19 during the provision of services.
41
This
includes practical guidance and updated advice
to informal carers on how to support persons
with disabilities in a manner safe for everyone.
Expand community support for persons
with disabilities. The growth in demand for
support services in the community without a
corresponding supply of services can increase
pressure on families to provide unpaid,
informal care, with negative consequences
on both persons with disabilities and
family members, particularly women.
42
In Argentina, Peru, Spain and other countries,
for instance, persons who provide support
to people with disabilities are exempted
from restrictions of movement and physical
distancing.
43
Community support networks
40 OHCHR, Covid-19 and the Rights of Persons with Disabilities: Guidance, May 2020
41 WHO, Disability considerations during the COVID-19 outbreak, March 2020
42 C. Devandas, UN Special Rapporteur on the rights of persons with disabilities, Access to rights-based support for persons with
disabilities, UN Doc. A/HRC/34/58, 2016.
43 Argentina, Decree 297/2020, Article 6.5.; Spain Real Decree 463/2020; Peru Supreme Decree No 044-2020-PCM.

POLICY BRIEF: A DISABILITY-INCLUSIVE RESPONSE TO COVID-19 13
have also developed in Colombia and other
countries which recruit volunteers that support
persons with disabilities and older persons
with their groceries and other purchases.
44
SOCIAL PROTECTION
AND EMPLOYMENT
Social protection has already proven a key
element in the immediate relief to be provided
to persons affected by the socio-economic
impact of the crisis.
45
It is particularly relevant
for persons with disabilities out of work, who
have lost their job or their income resulting
from the informal economy, all of which are
at risk of poverty and extreme poverty.
Expand mainstream and disability-targeted
social protection and adapt delivery
mechanisms to provide adequate relief and
support to persons with disabilities and their
families. This can be done by: advancing and/
or increasing payments of disability benets;
extending coverage to persons with disabilities
already registered but who were not previously
eligible, and through (online) registration of
persons with disabilities; providing disability
top-ups to beneciaries of mainstream social
assistance schemes, including to family
members who have to stop work to support
persons with disabilities; and establishing
electronic payment and home delivery for
cash and essential food and non-food items.
Employment and working conditions need to
be responsive to accessibility and inclusion.
Persons with disabilities who continue working,
whether essential workers or others, may
need specic protection or adjustments to
stay safe during the pandemic. At all times it
is important that employers and workplaces
provide accessible environments and
reasonable workplace adjustments based
on individual needs. Persons with disabilities
who own businesses or work in the informal
economy may need particular support to
be able to maintain their livelihoods.
Alternate working arrangements and conditions
made accessible and inclusive. Platforms and
new ways of meeting must be accessible to all,
and adequate adjustments put in place to allow
persons with disabilities to work from home.
44 Such practice is promoted by States, such as Colombia.
45 United Nations, Shared Responsibility, Global Solidarity: Responding to the Socio-Economic Impacts of Covid-19, March 2020
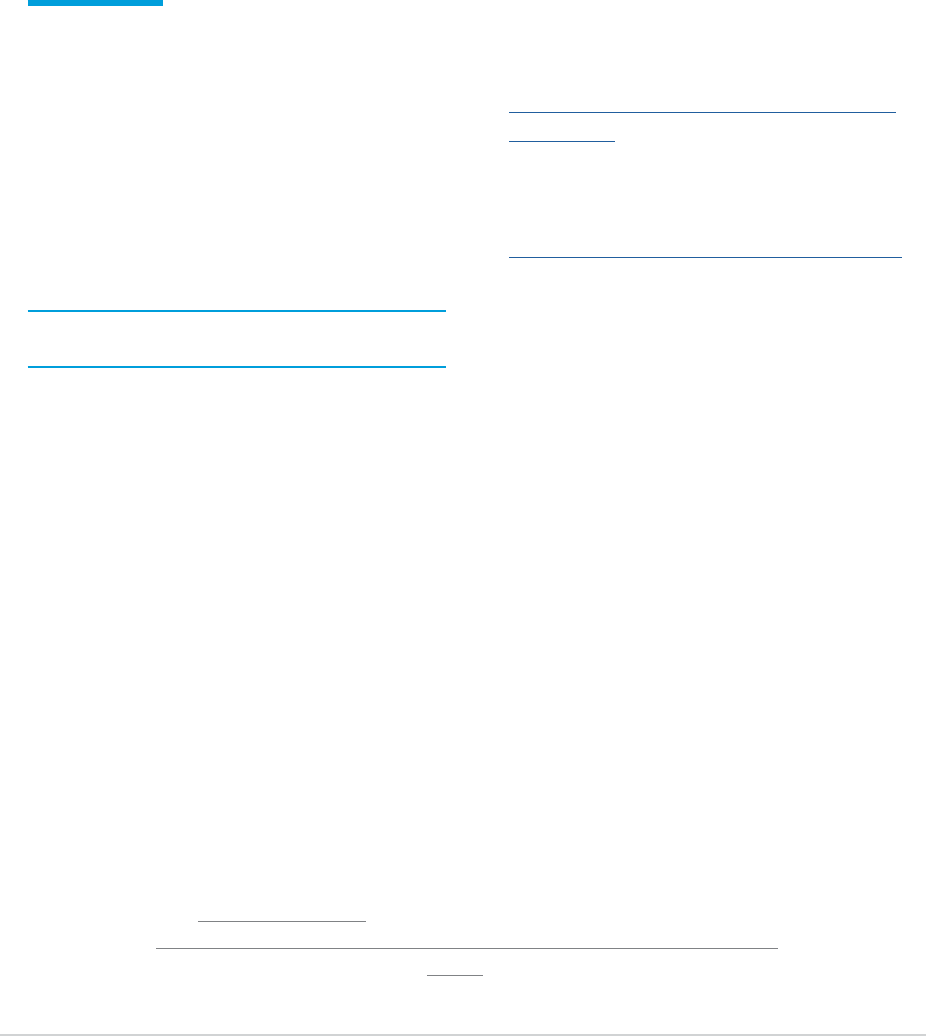
Figure 3 Employment-to-population ratios, for persons aged 15 years and over by disability status and sex, 2006-2016

14 POLICY BRIEF: A DISABILITY-INCLUSIVE RESPONSE TO COVID-19
Ensure disability-inclusive Occupational
Health and Safety (OSH) measures. New OSH
measures may apply particularly to persons
with disabilities. In such cases, different
arrangements may be required, such as priority
to work from home or placed in paid leave.
Approaches to coming out of lockdown need
to be sensitive to the particular situation
of persons with disabilities. Persons with
disabilities and their family members or
support services have different levels of
vulnerability to COVID-19. Some persons
with disabilities, including older persons
with disabilities, may need to isolate for
longer than other groups. Social protection
and working arrangements need to be
adaptive to support their ability to do this.
The International Labour Organization (ILO)
has developed a guidance note on socio-
economic actions for persons with disabilities.
Information is also available on: Disability
inclusion in COVID-19 and the world of work
and Social protection measures for persons
with disabilities in the COVID-19 crisis.
EDUCATION
Students with disabilities are likely to face
greater barriers in accessing distance learning
or rejoining classes once they are available,
and face increased risk of dropping out of
education during disruptions to learning.
Ensure distance learning is accessible to,
and inclusive of, students with disabilities.
Education actors need to take measures to
ensure continuity of learning for students with
disabilities and return to school programmes.
This may include providing specialized
equipment to support their learning, including
assistive technology and devices, and
support to caregivers/parents of children with
disabilities. UNICEF has produced a guidance
note for staff and partners on supporting the
learning of children in areas of school closures,
which includes guidance on making learning
accessible to children with disabilities.
46
Address impacts that go beyond learning. For
many children with disabilities, peer relations,
social perception and social competence are
signicant aspects of their Individual Education
Plans, all of which are challenged in the context
of school closures. School closings can also
mean that many children with disabilities will
not access complementary services,
47
such
as food and medical check-ups, or referral
mechanisms for abuse and neglect.
Ensure that return to school programmes
are inclusive. Education actors need to
ensure that return to school programmes are
inclusive of children and young persons with
disabilities, in recognition of the increase
in the learning/achievement gap. This may
include development of plans for accelerated
education, remedial, and catch-up programmes.
46 UNICEF, All Means All – How to support learning for the most vulnerable children in areas of school closures, 2020
47 United Nations, Policy Brief: The impact of COVID-19 on Children, April 2020

POLICY BRIEF: A DISABILITY-INCLUSIVE RESPONSE TO COVID-19 15
PREVENTION OF AND
RESPONSE TO VIOLENCE
Persons with disabilities often face incidents of
violence in situations of isolation, with women
and girls with disabilities at even higher risk.
48
Reporting and access to domestic violence
services and assistance are particularly
challenging, as these are commonly not inclusive
of, nor accessible to persons with disabilities.
Ensure inclusive and accessible victim
assistance services. It is important to ensure
that reporting mechanisms and access to
victim assistance services are accessible to
persons with disabilities.
49
Being proactive and
innovative in outreach to those who are isolated,
including through voluntary networks, has
proven to be a key measure, as well as ensuring
that online counseling and other technology-
based solutions are accessible and respond
to the diversity of people with disabilities.
Strengthen awareness raising and knowledge.
Building capacity of services and communities
to prevent disability-related violence is key, as
is promoting awareness-raising about violence
against persons with disabilities, particularly
women and girls. For example, UN Women
Papua New Guinea is working with partners
to integrate COVID-19 aspects to improve
quality and standards for counselling and case
management services that will particularly target
women with disabilities. Women with disabilities
are being supported to run campaigns on
ending violence against women in a pandemic.
HUMANITARIAN CONTEXTS
Persons with disabilities in humanitarian and
disaster contexts face specic and heightened
challenges in the COVID-19 outbreak: barriers to
implementing basic hygiene measures; physical
distancing limitations in high-density sites;
barriers to accessing health care on the basis
of both disability and legal status, which may
determine and restrict their access to health care
and other services.
50
The Inter-Agency Standing
Committee (IASC) Guidelines on Inclusion
of Persons with Disabilities in Humanitarian
Action provide detailed sectoral information for
stakeholders working in humanitarian contexts.
51
Ensure disability-inclusive humanitarian
assistance and disaster response. National
and local coordination mechanisms, as well
as Preparedness and Response Plans need
to be disability-inclusive. In particular, it is
important to ensure that Humanitarian Response
Plans factor in responses targeted towards
persons with disabilities, including in WASH,
health, and food and nutrition, with adequate
resourcing, monitoring and adjustment, as
required. Concrete adaptions in humanitarian
assistance could include, for example, improving
accessibility of WASH facilities; distribution of
additional or disability-specic hygiene items
and supplies; targeted shelter assistance
for at-risk individuals to allow for physical
distancing; in-kind provision of goods, cash and
voucher assistance, and direct service provision;
and providing alternative arrangements
for food and non-food items distribution to
households of persons with disabilities.
48 S. Hellum Braathen, P. Rohleder and G. Azalde, “Sexual and reproductive health and rights of girls with disabilities: a review of the
literature”, SINTEF, 2017.
49 United Nations, Policy Brief: Impact of COVID-19 on Women, April 2020
50 See also references to persons with disabilities in the UN-led COVID-19 Global Humanitarian Response Plan, March 2020
51 Inter-Agency Standing Committee, IASC Guidelines on Inclusion of Persons with Disabilities in Humanitarian Action, 2019

16 POLICY BRIEF: A DISABILITY-INCLUSIVE RESPONSE TO COVID-19
Everything we do during and after the
COVID-19 crisis must have a strong focus on
building more equal, inclusive and sustainable
economies and societies that are more
resilient in the face of pandemics and the
many other global challenges we face.
Countries’ immediate efforts towards social
and economic recovery will be crucial for
progress towards the Sustainable Development
Goals (SDGs), including addressing inequalities
and ensuring that no one is left behind
52
.
While building back better
53
, it is critical that
persons with disabilities are part and parcel
of the response which countries, often with
the support of the UN, are preparing. These
responses, if well designed, can address
the exclusion and discrimination faced by
persons with disabilities, thus creating more
resilient communities and systems.
To build equal, inclusive and resilient
communities it is important to:
1. Meaningfully engage persons with
disabilities at all stages of the response:
When supporting local initiatives,
governments, UN entities, international
donors and civil society organizations
need to promote, fund and monitor the
inclusion of persons with disabilities in
all stages of design and implementation
of the relevant measures.
2. Prioritize persons with disabilities in
the socio-economic response: National
and sub-national economic models and
assumptions need to be critically reviewed
to identify gaps that disproportionately
impact persons with disabilities and
take into account the cost of under-
investment in disability-inclusion.
3. Track inclusion and empowerment of
persons with disabilities in national
response and recovery plans: A long-term
inclusive response needs to be closely
tied to inclusive national development
planning and nancing processes.
Disability inclusion should be a requirement
in all COVID-19 actions and systems
to allow tracking and accountability
(e.g. OECD DAC disability marker).
54
4. Improve health outcomes for persons
with disabilities: This entails building
accessible health systems, rights-based
training of health personnel and ensuring
universal health coverage for persons with
disabilities as a cornerstone for achieving
the health-related SDG targets. Further,
improving the determinants of health
for persons with disabilities is critical.
5. Build sustainable and disability-
inclusive social protection systems:
Universal disability allowances across
the life cycle addressing disability-related
5. Delivering on the SDGs —
Building Back Better
52 United Nations, A UN framework for the immediate socio-economic response to COVID-19, April 2020
53 United Nations, Sendai Framework for Disaster Risk Reduction 2015-2030, 2015
54 OECD, Handbook for the marker for the inclusion and empowerment of persons with disabilities, 2019

POLICY BRIEF: A DISABILITY-INCLUSIVE RESPONSE TO COVID-19 17
extra costs should be designed so that
these are compatible with employment
and other social assistance schemes
aiming at basic income security.
6. Address the specic situation of workers
with disabilities in all sectors: Stimulus
packages, including those that will promote
training and jobs in the transition to a green
economy should explicitly include persons
with disabilities in general, as well as women
and youth with disabilities in particular.
7. Invest in community-based solutions
now: Particular attention needs to be
given to persons with disabilities living in
residential institutions and funds should be
used to initiate, accelerate and complete
deinstitutionalization strategies and
transition to community-based solutions.
This includes investing and developing
support services and implementing
inclusive services at local level, such as
education and primary health care, including
rehabilitation, as cornerstones for achieving
the SDG targets for persons with disabilities.
8. Initiate multi-stakeholder dialogue and
collaboration: Inter-sectoral linkage is
required to address the multi-dimensional
nature of disability and the inter-
sectoral response that is necessary.
Bringing together all stakeholders—
government, UN entities, private sector,
organizations of persons with disabilities
and broader civil society—in the design,
implementation and monitoring of the
long-term rebuilding plan will be critical.

18 POLICY BRIEF: A DISABILITY-INCLUSIVE RESPONSE TO COVID-19
6. Conclusion
COVID-19 has created a human crisis of
unprecedented scale, which is disproportionately
impacting one billion people with disabilities.
This requires an unprecedented response—an
extraordinary scale-up of support and political
commitment—to ensure that people with
disabilities have access to essential services,
including to immediate health and social
protection services, to tide over the crisis.
A disability inclusive COVID-19 response and
recovery will better serve everyone. It will
provide for more inclusive, accessible and agile
systems capable of responding to complex
situations, reaching the furthest behind rst.
It will pave the way for a better future for all.
