Policy Brief for Heads of Government
The Global Impact of Dementia 2013–2050

ALZHEIMER’S DISEASE INTERNATIONAL · THE GLOBAL VOICE ON DEMENTIA
Introduction
Alzheimer’s Disease International (ADI) published
global prevalence data on dementia in the World
Alzheimer Report 2009
1
based on a systematic
review of 154 studies conducted worldwide, and
United Nations population projections through to
the year 2050. We estimated 36 million people with
dementia in 2010, nearly doubling every 20 years to
66 million by 2030 and to 115 million by 2050.
Key findings included
• 58% of those affected lived in low and middle
income countries, underlining the high impact of
the condition in those regions, where awareness
is low, health and social care are poorly
developed and social protection is limited.
• Population ageing is the main driver of projected
increases.
• We assumed that age-specific prevalence
would remain constant. This assumption is
challenged by recent evidence suggesting a
modest recent decline in dementia prevalence
in some higher income countries (HIC), but an
increase in prevalence in China, likely linked to
recent changes in population health, particularly
exposure to cardiovascular risk factors.
• Since population ageing is occurring at an
unprecedentedly fast rate in middle income
countries, the bulk of the increase in numbers
through to 2050 will occur in those regions. By
2050 71% of those with dementia would be living
in what are currently lower and middle-income
countries (LMIC).
The Global Impact of Dementia 2013–2050
Although high income countries, including the G8, have borne the brunt of the dementia
epidemic, this is a global phenomenon. Most people with dementia live in low and
middle income countries, and most of the dramatic increases in numbers affected,
through to 2050, will occur in those regions. In a spirit of international cooperation and
solidarity we urge the G8 governments to sponsor intergovernmental action to make
dementia a global priority. Crucially, this must include opening up access to diagnosis
and current evidence-based treatment and care. All countries worldwide are failing in
this basic objective. Action to address this problem should be balanced, as a priority,
with research to improve treatment options and quality of care.
Since 2009, the global evidence base has
expanded, most particularly with a new
systematic review of the prevalence of
dementia in China
3
comprising 75 studies,
most published in Chinese language journals,
and with seven studies from five sub-
Saharan African countries, where previously
only one study from Nigeria had been
available.
The G8 Dementia Summit on 11 December
2013 provides a timely opportunity to
reassess and update evidence on the scale
and the distribution of the global dementia
epidemic, in particular its impact on more
developed (G8, G20, OECD and ‘high
income’ countries) and less developed ‘low
and middle income’ countries.
For the current update, we carried out a
limited review, focusing on the new evidence
emerging from China and the sub-Saharan
African regions, and applied the new
prevalence proportions to the latest (2012)
UN population projections
2
. Details of the
methodology are provided in Annex 1.
The work on this report has been a joint
effort of the Global Observatory for Ageing
and Dementia Care (Prof Martin Prince,
Dr Maëlenn Guerchet and Dr Matthew Prina),
and the ADI office.
2
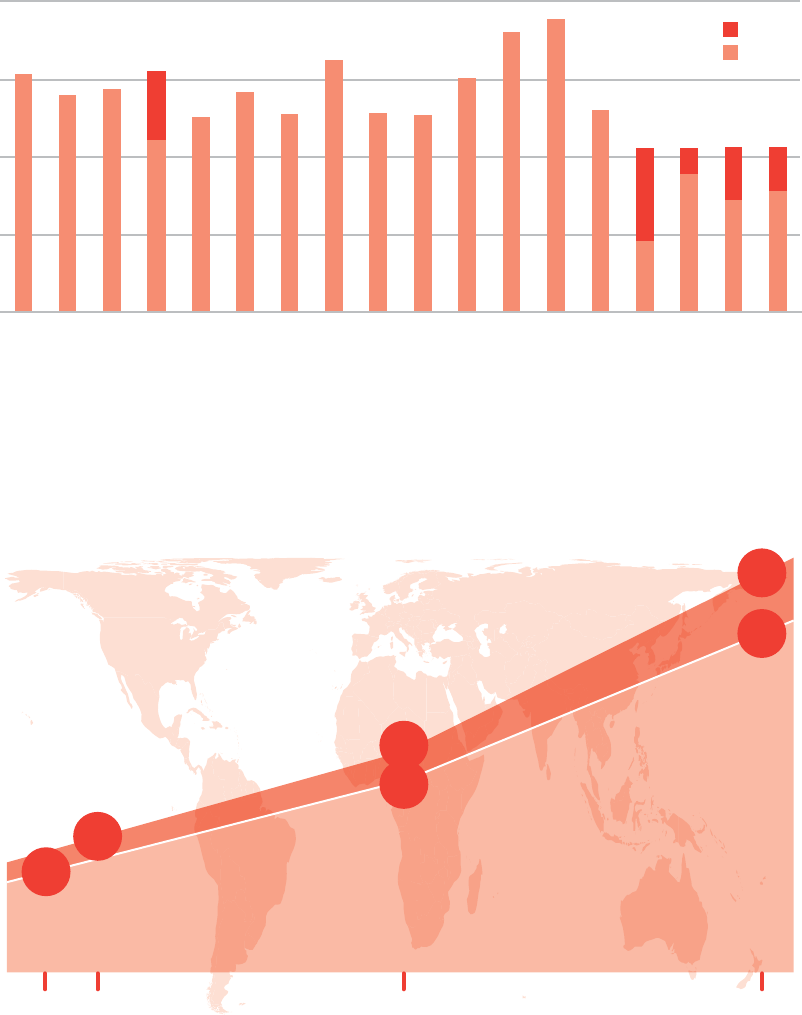
Figure 1 Original (2009 World Alzheimer Report) and updated age-specific prevalence of dementia (%) by region,
showing impact of new data from Asia East (China) and Sub-Saharan Africa
Results
The prevalences of dementia estimated from the
recent more comprehensive review and meta-
analysis of China studies
3
and our own meta-
analysis of studies from sub-Saharan Africa were
substantially higher than those used in the 2009
World Alzheimer Report. Age-standardised to a
standard West European population, prevalence
for East Asia increased from 4.98% to 6.99%
and in the sub-Saharan African regions from a
range of 2.07% to 4.00%, to 4.76% (Figure 1).
The net effect, as more data becomes available,
is to further reduce the variation in prevalence
between world regions.
The number of people living with dementia
worldwide in 2013 is estimated at 44.35 million,
reaching 75.62 million in 2030 and 135.46 million
in 2050 (Figure 2). The updated estimates are
higher than our original estimates reported in the
2009 World Alzheimer Report, by 15% in 2030,
and by 17% in 2050.
0
2
5
7
9
Australasia
Asia Pacific
Oceania
Asia E
Asia S
Asia SE
Asia Central
Europe W
Europe Central
Europe E
America N
Caribbean
Latin America
N Africa/ Middle East
SSA W
SSA E
SSA Central
SSA S
Standard Prevalence (%)
Updated
Original
0
35
70
105
140
2010 2013 2030 2050
Original
Updated
People with dementia (millions)
36
million
66
million
115
million
44
million
76
million
135
million
Figure 2 Increase in numbers of people with dementia worldwide (2010-2050), comparing original and
updated estimates
3POLICY BRIEF FOR HEADS OF GOVERNMENT: THE GLOBAL IMPACT OF DEMENTIA 2013–2050
ALZHEIMER’S DISEASE INTERNATIONAL · THE GLOBAL VOICE ON DEMENTIA
The largest increases in projected numbers of
people with dementia are those for the Asia East
and Sub-Saharan African regions, accounted
for by the higher age-specific prevalence of
dementia estimated in our new reviews of survey
data from those regions (Annex 2). Hence, in
2050 we are now estimating 33.61 million people
with dementia in Asia East (an increase of 49%
from the previous estimate of 22.54 million) and
5.05 million older people with dementia in SSA
(an increase of 136% from the previous estimate
of 2.14 million). However, the new estimates of
numbers of people with dementia are higher for
all GBD regions than those estimated in 2009.
This is explained by the underestimation of
current numbers of older people in the previous
UN population estimates (affecting the 2013
figures), and revision upwards of probability of
survival into older age (affecting the 2030 and
2050 projections).
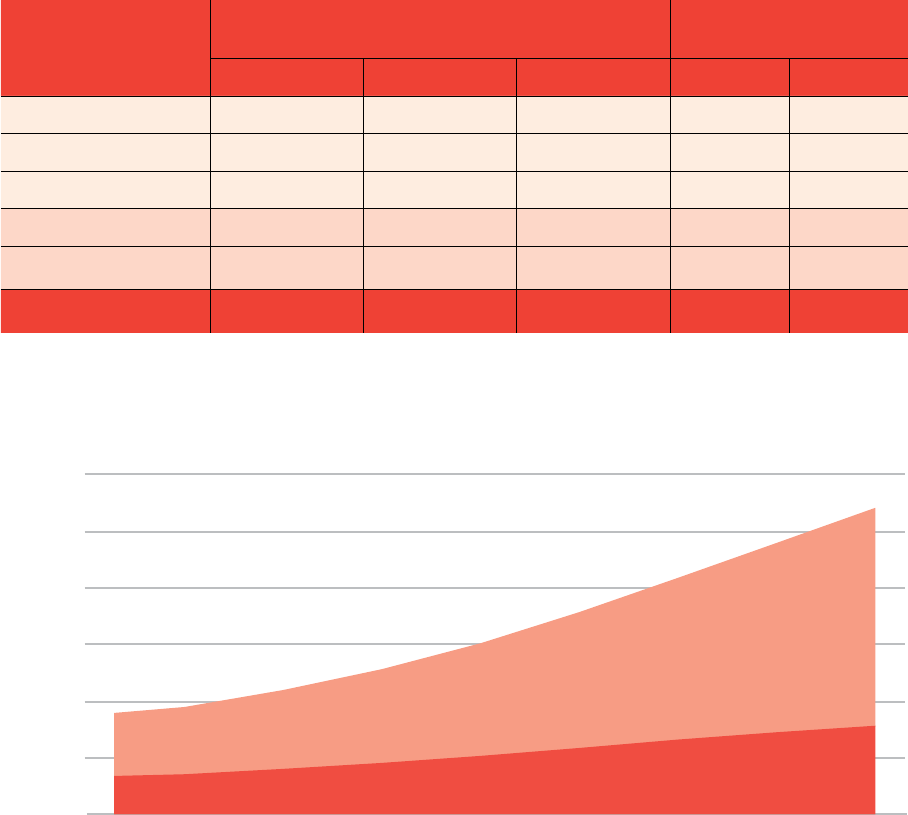
We now estimate that while 32% of people
with dementia live in G8 countries and 38%
in high income countries, 62% live in low and
middle income countries (Table 1). By 2050, the
proportion living in G8 countries will have shrunk
to 21%, while the proportion living in what are
currently low and middle income countries will
have increased to 71%.
Region
People with dementia millions
(% of world total)
Proportionate increase
(%)
2013 2030 2050 2013-2030 2013-2050
G8 14.02 (32%) 20.38 (27%) 28.91 (21%) 45 106
G20 33.93 (76%) 56.40 (75%) 96.61 (71%) 66 185
OECD 18.08 (41%) 27.98 (37%) 43.65 (32%) 55 142
High income 17.00 (38%) 25.86 (34%) 39.19 (29%) 52 131
Low and middle income 27.84 (62%) 49.76 (66%) 96.27 (71%) 79 246
World 44.35 75.62 135.46 71 205
0
25
50
75
100
125
150
2013 2015 2020 2025 2030 2035 2040 2045 2050
Low and middle income countries
High income countries
Millions of people with dementia
Year
Table 1 Updated estimates of the number of people with dementia living in G8, G20,
OECD, LMIC and HIC countries, and as a percentage of world total
Figure 3 Number of people with dementia in low and middle income countries
compared to high income countries
4
diagnosis; case management across the
course of the illness; support, education and
training for carers; optimising physical health;
acetylcholinesterase inhibitors; cognitive
stimulation; and non-pharmacological
interventions for behavioural disturbance.
Currently less than half of those in high
income countries and fewer than 10% of
those in LMIC have received a dementia
diagnosis.
8 There are lessons to be drawn from the
HIV epidemic. First, new and dramatically
effective treatments can only be scaled up
when diagnostic and care systems are well
established. Second, affordable access
to new diagnostic technologies and drug
therapies will need rapidly to be extended
to low and middle income country markets,
where most of those who might benefit live.
Third, those countries that where involved
in ‘global trials’ should also benefit from
treatments being made available at subsidised
cost with adequate standards of care in place.
9 ADI and the World Health Organization have,
in their joint report Dementia: a public health
priority
13
, called upon all Governments to
make dementia a public and health priority. As
part of this process, all governments should
initiate national debates regarding the future
provision and financing of long-term care
(see World Alzheimer Report 2013: Journey
of Caring
15
). However, most are woefully
unprepared for the dementia epidemic with
only 13 countries having funded and sought to
implement a national dementia plan. Without
a plan, the risk is that health and social care
systems will not cope with the increase
in numbers and operate in crisis mode,
escalating costs even further.
10 At the eve of the G8 Dementia Summit in
London, UK, it is not just the G8 countries,
but all nations that must commit to a
sustained increase in dementia research and
a comprehensive plan for collaborative action
involving all relevant government sectors,
industry and civil society. International
cooperation will be essential. There is a
need for a collaborative, global action plan
for governments, industry and non-profit
organisations like Alzheimer associations.
Priorities include; breaking down barriers to
effective research; promoting rapid translation
and ensuring equitable access to promising
technologies and treatments; technical
support for policymaking, health and social
care service and system development.
1 Dementia, including Alzheimer’s disease,
is one of the biggest global public health
challenges facing our generation. Newly
available data suggests that the current
burden and future impact of the dementia
epidemic has been underestimated,
particularly for the Asia East and Sub-Saharan
African regions.
2 This is a global epidemic – although cases
are disproportionately concentrated in the
world’s richest and most demographically
aged countries, already the clear majority
(62%) of people with dementia live in low and
middle income countries where access to
social protection, services, support and care
are very limited.
3 In the next few decades, the global burden
of dementia will shift inexorably to poorer
countries, particularly rapidly developing
middle income countries that are members of
the G20, but not the G8.
4 The future scale of the dementia epidemic
may be blunted through improvements in
population health, but our best estimates
suggest that only up to 10% of incidence
may thus be avoided
13
. Public health and
disease control measures targeting smoking,
underactivity, obesity, hypertension and
diabetes should be prioritised. Education and
other factors that enhance brain and cognitive
development will also improve the brain health
of those entering old age, and reduce the
incidence of dementia in late life.
5 Standard & Poor’s has described global
population ageing as the biggest threat to
the sustainability of sovereign debt. Among
the chronic diseases, dementia makes by far
the largest single contribution to disability
and needs for care among older people. The
current (2010) global societal economic cost
of dementia is US$ 604 billion, or 1% of global
GDP
14
. Costs will escalate proportionately
with numbers affected, and with increased
demand for formal care services, particularly
in low and middle income countries
13
.
6 Research must be a global priority if we
are to improve the quality and coverage of
care, find treatments that alter the course of
the disease, and identify more options for
prevention.
7 Investment in the search for a cure must be
balanced with initiatives to improve access
to currently available evidence-based
packages of care – these include timely
Conclusions and implications
5POLICY BRIEF FOR HEADS OF GOVERNMENT: THE GLOBAL IMPACT OF DEMENTIA 2013–2050
ALZHEIMER’S DISEASE INTERNATIONAL · THE GLOBAL VOICE ON DEMENTIA
Estimation of the number of people with
dementia
The new rates were applied to the new UN population
estimates for each 5-years age band (60-64, to 100 and
over)
2
. When rates were not available for one age-band
(i.e. over 90 in SSA and over 100 in China), the rate of
the nearest age-band was applied. As gender-specific
estimates were available neither for China nor SSA,
we applied the age-specific estimates to the whole
population and to each gender separately. In the East Asia
region – composed of China, Hong Kong SAR, Macao
SAR, Chinese Taipei and DPR Korea – the new rates were
applied to mainland China, Hong Kong SAR and Macao
SAR, whereas the East Asia rates from the 2009 Word
Alzheimer Report were maintained for the DPR Korea and
Chinese Taipei.
For Sub-Saharan Africa, the new rates were applied to
the countries belonging to the following Global Burden
Disease (GBD) regions: SSA West, SSA Central, SSA East
and SSA Southern. Based on the GBD regions, Algeria
belongs to the North Africa / Middle East, so we therefore
applied the EMRO B rates that are used for some of its
neighbours.
For all the other regions, we applied the rates found in
the 2009 World Alzheimer Report to the new population
estimates from the United Nations
2
.
Annex 1: Methods
The prevalence of dementia in China and
Sub-Saharan Africa
The estimates for China were revised based on the recent
meta-analysis published by Chan et al.
3
. This meta-
analysis included reports for dementia or Alzheimer’s
Disease in mainland China, published in Chinese and
English between 1990 and 2010. The rates applied to the
population estimates were the age-specific prevalence of
dementia in 2010. A new systematic review of dementia
in China has also been recently published
4
, together with
a new large multi-centre population-based prevalence
study of dementia in China
5
. These studies were not
taken into account in our estimates, but will be included in
any future updates.
For Sub-Saharan Africa, we conducted a systematic
review of the literature on the prevalence of dementia with
Pubmed / Medline up to October 2013 using a similar
methodology and inclusion criteria that we used for the
2009 World Alzheimer Report
1
(see online appendix).
We sought and included population-based studies of the
prevalence of dementia among people aged 60 years
and over for which the fieldwork started on or after 1st
January 1980. Prevalence rates were extracted for seven
studies covering five different countries
6 -12
. A random
effect exponential (Poisson) model was used to assess
the effects of age on the prevalence of dementia. We
then applied the relevant mean ages to the coefficients
estimated from the model, to estimate prevalence in five
year age-bands from 65-69 years to 85 years and over,
for both sexes combined.
References
1 Alzheimer’s Disease International: World Alzheimer
Report 2009. 2009.
2 United Nations Department of Economic and
Social Affairs Population Division: World Population
Prospects: The 2012 Revision, DVD Edition. 2013.
3 Chan KY, Wang W, Wu JJ, Liu L, Theodoratou E, Car
J, Middleton L, Russ TC, Deary IJ, Campbell H et al:
Epidemiology of Alzheimer’s disease and other forms
of dementia in China, 1990-2010: a systematic review
and analysis. The Lancet 2013, 381(9882):2016-2023.
4 Wu YT, Lee HY, Norton S, Chen C, Chen H, He C,
Fleming J, Matthews FE, Brayne C: Prevalence
studies of dementia in mainland china, Hong Kong
and taiwan: a systematic review and meta-analysis.
PLoS ONE 2013, 8(6):e66252.
5 Jia J, Wang F, Wei C, Zhou A, Jia X, Li F, Tang M, Chu
L, Zhou Y, Zhou C et al: The prevalence of dementia
in urban and rural areas of China. Alzheimers Dement
2013.
6 Hendrie HC, Osuntokun BO, Hall KS, Ogunniyi AO,
Hui SL, Unverzagt FW, Gureje O, Rodenberg CA,
Baiyewu O, Musick BS: Prevalence of Alzheimer’s
disease and dementia in two communities: Nigerian
Africans and African Americans. Am J Psychiatry
1995, 152(10):1485-1492.
7 Guerchet M, Houinato D, Paraiso MN, von Ahsen
N, Nubukpo P, Otto M, Clement JP, Preux PM,
Dartigues JF: Cognitive impairment and dementia
in elderly people living in rural Benin, west Africa.
Dement Geriatr Cogn Disord 2009, 27(1):34-41.
8 Guerchet M, M’Belesso P, Mouanga AM, Bandzouzi B,
Tabo A, Houinato DS, Paraiso MN, Cowppli-Bony P,
Nubukpo P, Aboyans V et al: Prevalence of dementia in
elderly living in two cities of Central Africa: the EDAC
survey. Dement Geriatr Cogn Disord 2010, 30(3):261-268.
9 Paraiso MN, Guerchet M, Saizonou J, Cowppli-Bony
P, Mouanga AM, Nubukpo P, Preux PM, Houinato DS:
Prevalence of dementia among elderly people living
in Cotonou, an urban area of Benin (West Africa).
Neuroepidemiology 2011, 36(4):245-251.
10 Yusuf AJ, Baiyewu O, Sheikh TL, Shehu AU: Prevalence
of dementia and dementia subtypes among community-
dwelling elderly people in northern Nigeria. Int
Psychogeriatr 2011, 23(3):379-386.
11 Longdon AR, Paddick SM, Kisoli A, Dotchin C, Gray
WK, Dewhurst F, Chaote P, Teodorczuk A, Dewhurst M,
Jusabani AM et al: The prevalence of dementia in rural
Tanzania: a cross-sectional community-based study. Int J
Geriatr Psychiatry 2013, 28(7):728-737.
12 Guerchet M, Banzouzi-Ndamba B, Mbelesso P, Pilleron
S, Clement J-P, Dartigues J-F, Preux P-M.: Prevalence of
dementia in two countries of Central Africa: comparison
or rural and urban areas in the EPIDEMCA study.
Neuroepidemiology 2013, 41:223-316.
13 World Health Organization and Alzheimer’s Disease
International, Dementia: a public health priority, Geneva
April 2012, http://www.alz.co.uk/WHO-dementia-report
14 Wimo A, Prince M. World Alzheimer Report 2010; The
Global Economic Impact of Dementia. 2010. London,
Alzheimer’s Disease International
15 World Alzheimer Report 2013, Journey of Caring, An
analysis of long-term care for dementia, http://www.alz.
co.uk/research/world-report-2013
6
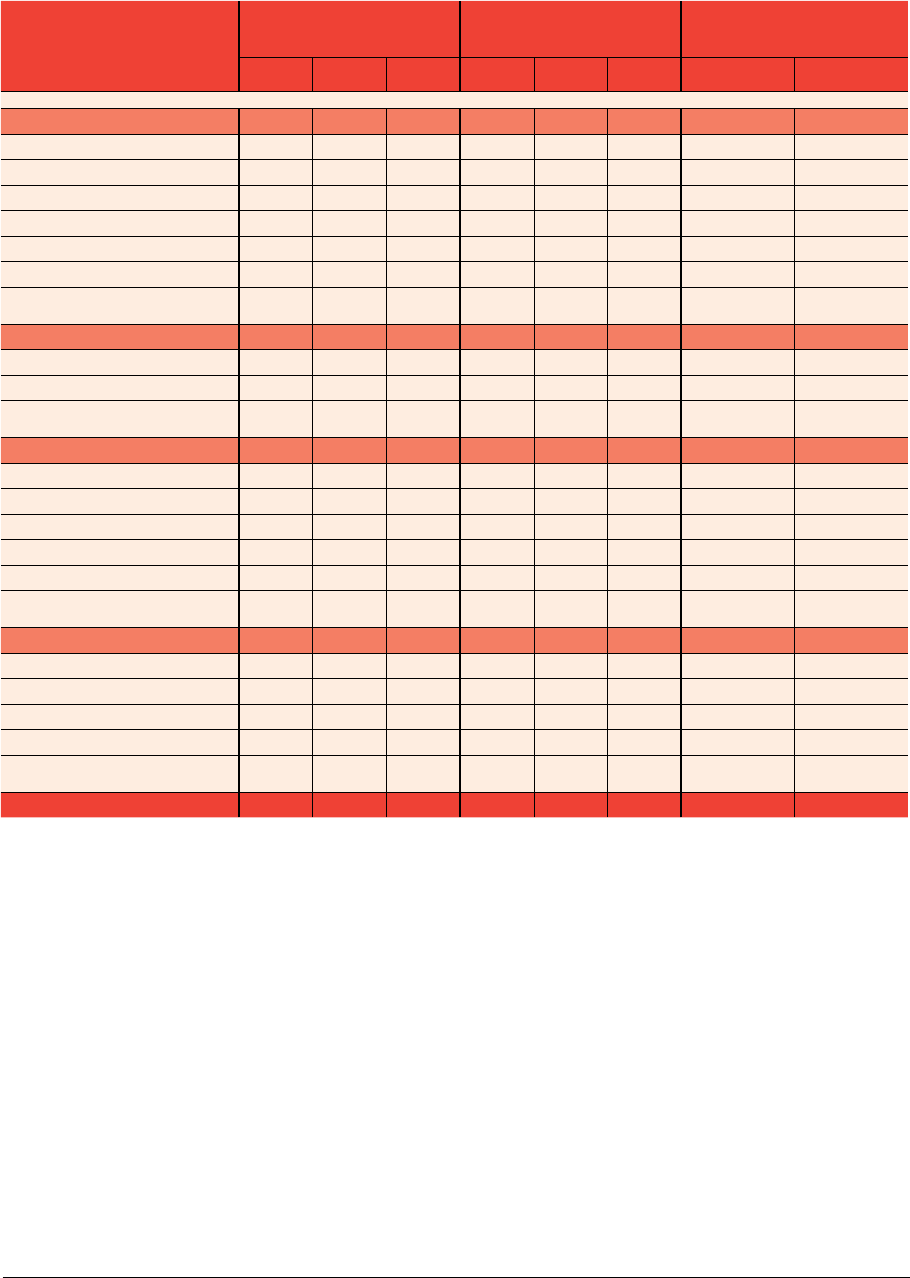
Annex 2
GBD Region
Original estimates (2009) Updated estimates
Proportionate increases
(%) for new estimates
2010 2030 2050 2013 2030 2050 2013- 2030 2013- 2050
Asia/Pacific 15.94 33.04 60.92 21.87 39.79 71.84 82 228
Australasia 0.31 0.53 0.79 0.37 0.62 1.02 68 176
Asia Pacific High Income 2.83 5.36 7.03 3.26 5.50 7.58 69 133
Oceania 0.02 0.04 0.10 0.02 0.04 0.09 100 350
Asia Central 0.33 0.56 1.19 0.29 0.44 0.88 52 203
Asia East 5.49 11.93 22.54 10.46 18.83 33.61 80 221
Asia South 4.48 9.31 18.12 4.74 8.50 16.61 79 250
Asia Southeast 2.48 5.30 11.13 2.74 5.87 12.05 114 340
Europe 9.95 13.95 18.65 10.93 14.8 20.75 35 90
Europe Central 1.10 1.57 2.10 1.23 1.69 2.29 37 86
Europe Eastern 1.87 2.36 3.10 1.86 2.03 2.44 9 31
Europe Western 6.98 10.03 13.44 7. 8 4 11.08 16.02 41 104
The Americas 7.82 14.78 27.08 8.77 15.8 30.51 80 248
North America High Income 4.38 7.13 11.01 4.58 7.28 11.74 59 156
Caribbean 0.33 0.62 1.04 0.38 0.63 1.14 66 200
Latin America Andean 0.25 0.59 1.29 0.31 0.64 1.46 106 371
Latin America Central 1.19 2.79 6.37 1.38 2.95 7.07 114 412
Latin America Southern 0.61 1.08 1.83 0.71 1.17 2.13 65 200
Latin America Tropical 1.05 2.58 5.54 1.42 3.13 6.97 120 391
Africa 1.86 3.92 8.74 2.78 5.24 12.35 88 344
North Africa / Middle East 1.15 2.59 6.19 1.47 2.91 7. 2 9 98 396
Sub-Saharan Africa Central 0.07 0.12 0.24 0.13 0.23 0.48 77 269
Sub-Saharan Africa East 0.36 0.69 1.38 0.55 1.06 2.45 93 345
Sub-Saharan Africa Southern 0.10 0.17 0.20 0.19 0.29 0.49 53 158
Sub-Saharan Africa West 0.18 0.35 0.72 0.44 0.76 1.63 73 270
World 35.56 65.69 115.38 44.35 75.62 135.46 71 205
Table 1 Numbers of people with dementia according to GBD regions (in millions, by year)
Acknowledgements
Authors
Prof Martin Prince *
Dr Maëlenn Guerchet *
Dr Matthew Prina *
Alzheimer’s Disease International
* Global Observatory for Ageing and Dementia Care,
Health Service and Population Research Department, King’s College London
Thanks to
Pr Richard Walker, Dr Catherine Dotchin and Dr William Keith Gray from the Northumbria Healthcare NHS Foundation
Trust, the Institute for Ageing and Health, and the Institute of Health and Society, in Newcastle University (UK) for providing
us prevalence rates from their study in Tanzania.
Pr Pierre-Marie Preux, from the UMR Inserm 1094 Tropical Neuroepidemiology in Limoges (France), and the EPIDEMCA
group, for allowing us to include their last results in Central Africa before their publication.
Cover image © Barbara Kinney, used with permission of Alzheimer’s Association (US).
Policy Brief for Heads of Government: The Global Impact of Dementia 2013–2050
Published by Alzheimer’s Disease International (ADI), London. December 2013
Copyright © Alzheimer’s Disease International
7POLICY BRIEF FOR HEADS OF GOVERNMENT: THE GLOBAL IMPACT OF DEMENTIA 2013–2050

ALZHEIMER’S DISEASE INTERNATIONAL · THE GLOBAL VOICE ON DEMENTIA
Alzheimer’s Disease International:
The International Federation
of Alzheimer’s Disease and
Related Disorders Societies, Inc.
is incorporated in Illinois, USA,
and is a 501(c)(3) not-for-profit
organization
Alzheimer’s Disease International
64 Great Suffolk Street
London SE1 0BL
UK
Tel: +44 20 79810880
Fax: +44 20 79282357
www.alz.co.uk
About Alzheimer’s Disease International
Alzheimer’s Disease International (ADI) is the international federation of Alzheimer
associations throughout the world. Each of our 79 members is a non-profit
Alzheimer association supporting people with dementia and their families.
ADI was founded in 1984 and registered as a non-profit organization in the USA.
Based in London, ADI is in official relations with the WHO since 1996 and has
consultative status with the UN since 2012.
ADI’s vision is an improved quality of life for people with dementia and their
families throughout the world. ADI aims to make dementia a global health priority,
to build and strengthen Alzheimer associations, and to raise awareness about
dementia worldwide. Stronger Alzheimer associations are better able to meet the
needs of people with dementia and their carers, and to be the global voice on
dementia.
Global Observatory for Ageing and Dementia Care
The Global Observatory for Ageing and Dementia Care, hosted at the Health
Service and Population Research Department, King’s College London, was
founded in 2013. Supported by Alzheimer’s Disease International and King’s
College London, the Observatory aims to synthesise global evidence for
policymakers and the public through high impact evidence-based reports for
Alzheimer’s Disease International (World Alzheimer Reports 2009, 2010, 2011 and
2013), the World Health Organization (Dementia; a public health priority) and other
relevant intergovernmental organisations. A particular focus is to identify and
promote effective innovations in health and social care policy and practice.
